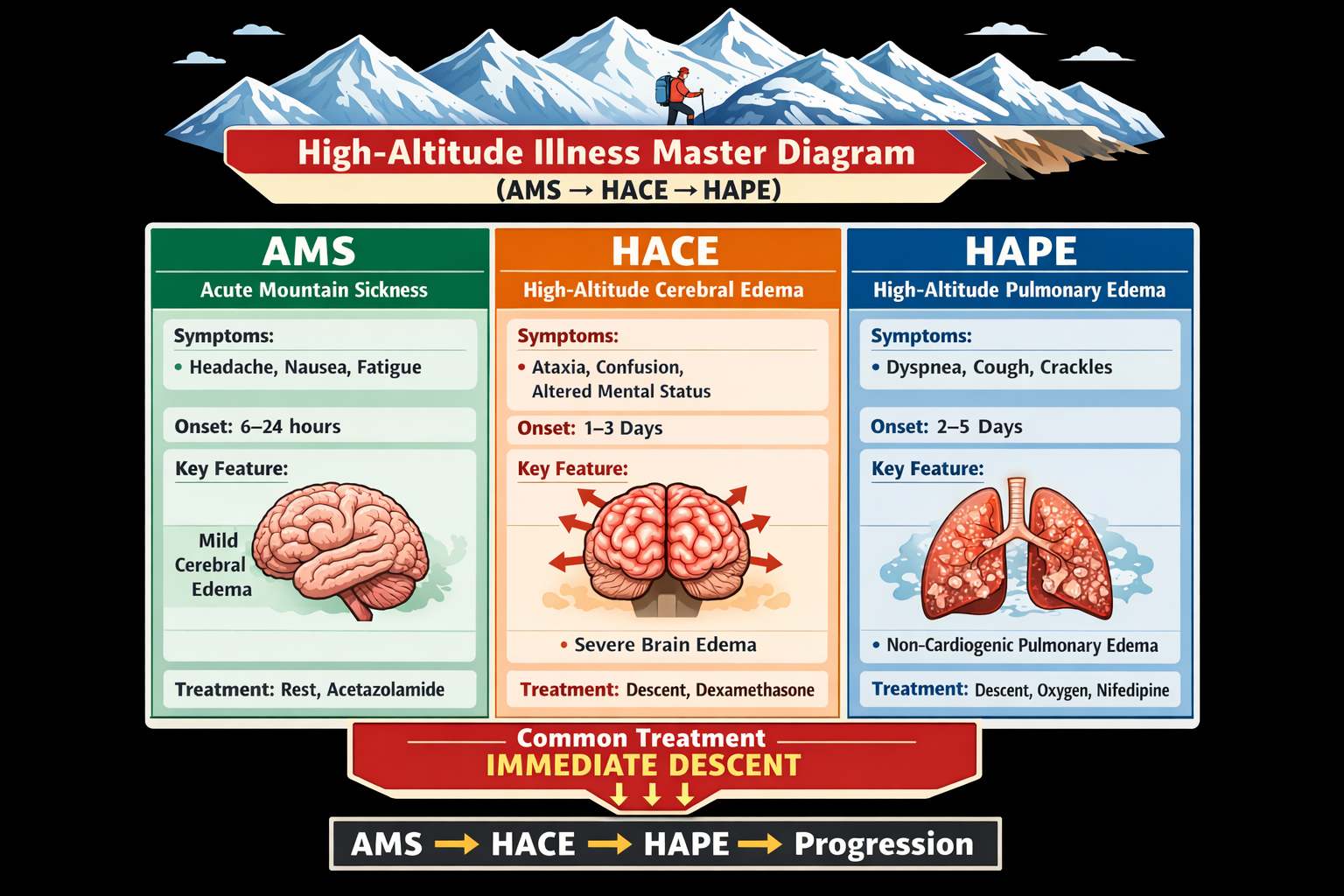
You’ve trained for months, packed your gear, and arrived at the trailhead—only to feel dizzy, nauseous, and exhausted within hours. No injury. No bug. Just altitude. Hiking altitude sickness affects thousands of outdoor enthusiasts every year, from weekend hikers to elite athletes. It’s not about fitness—it’s about oxygen. At elevations above 8,000 feet (2,438 m), the air thins dramatically, and your body struggles to adapt. Without proper acclimatization, acute mountain sickness (AMS) can escalate into life-threatening conditions like high-altitude pulmonary edema (HAPE) or high-altitude cerebral edema (HACE).
The good news? Hiking altitude sickness is predictable, preventable, and treatable. This guide gives you the tools to recognize early signs, manage symptoms, and return safely. Whether you’re hiking Mount Dana, trekking to Everest Base Camp, or flying into Cuzco, understanding how altitude affects your body could save your life. You’ll learn proven prevention strategies, medication dosing, and the one rule that overrides all others: descend when symptoms worsen.
Recognize Early Altitude Illness Signs
Spot Mild AMS Within 24 Hours
Acute mountain sickness (AMS) typically appears 6–24 hours after ascent and mimics a severe hangover. The most common sign is a headache unrelieved by ibuprofen, especially when combined with other symptoms. Key indicators include:
- Nausea or vomiting
- Dizziness or lightheadedness
- Fatigue beyond normal exertion
- Loss of appetite
- Insomnia or restless sleep
- Shortness of breath during mild activity
These symptoms often worsen at night due to reduced breathing during sleep. If you experience any combination, stop ascending immediately. Rest at your current elevation and hydrate. Most mild cases resolve in 1–3 days with no further gain in altitude.
Pro Tip: Use the Lake Louise Score (LLS)—a standardized symptom checklist—to track severity. A score of 3 or higher with headache confirms AMS.
Don’t Ignore These Warning Symptoms
Some signs signal progression beyond mild AMS. These are not normal and require urgent action:
- Headache that won’t go away despite medication
- Repeated vomiting
- Feeling worse after resting
- Inability to sleep even when exhausted
- Drowsiness or confusion
These may indicate advancing hypoxia and potential development of HACE or HAPE. Do not push through. Assume it’s altitude-related until proven otherwise.
Rule: “Don’t Go Up Until Symptoms Go Down”
This golden rule applies to all hikers. If you feel unwell at altitude, do not climb higher. Continuing upward increases risk exponentially. Instead:
- Pause your ascent
- Rest and rehydrate
- Monitor symptoms for 12–24 hours
- Descend if no improvement
Even a drop of 1,000 feet (305 m) can dramatically improve oxygen levels and relieve symptoms.
Identify Life-Threatening Altitude Emergencies
HAPE: Fluid in the Lungs
High-altitude pulmonary edema (HAPE) occurs when low oxygen causes blood vessels in the lungs to constrict and leak fluid. It usually develops 2–5 days after ascent, especially with overexertion or rapid gain in sleeping altitude.
Critical Symptoms:
- Shortness of breath at rest
- Persistent cough
- Coughing up frothy, watery, or pink-tinged sputum
- Chest tightness or heaviness
- Rapid heart rate (over 100 bpm at rest)
- Cyanosis (blue lips or fingernails)
- Extreme fatigue or weakness
Field Check: Recovery Time Test
After light exertion (e.g., walking 50 steps), time how long it takes your breathing and heart rate to return to baseline. If recovery takes more than 5 minutes, suspect HAPE.
Urgency Level: HAPE can be fatal within 12 hours if untreated. Immediate descent is mandatory.
HACE: Brain Swelling at Altitude
High-altitude cerebral edema (HACE) is the most dangerous form of altitude illness—essentially brain swelling caused by fluid leakage. It often follows untreated AMS but can occur independently.
Critical Symptoms:
- Headache unresponsive to painkillers
- Loss of coordination (ataxia)
- Confusion or disorientation
- Hallucinations or irrational behavior
- Drowsiness progressing to coma
- Difficulty waking up
Field Test: Tandem Gait
Ask the person to walk heel-to-toe in a straight line for 10 steps. Inability to do so is a strong indicator of HACE.
Urgency Level: HACE can cause death within 24 hours. Even one failed step means immediate descent required.
HAPE vs HACE: Know the Difference

| Feature | HAPE | HACE |
|---|---|---|
| Primary Organ Affected | Lungs | Brain |
| Onset Time | 2–5 days | 3+ days (or rapid ascent) |
| Key Symptom | Breathlessness at rest | Ataxia or confusion |
| Cough | Present (frothy) | Absent or mild |
| Mental Status | Alert (early) | Altered early |
Both are medical emergencies. No field treatment replaces descent.
Prevent Altitude Sickness Before It Starts
Ascend Slowly Above 8,000 Feet
The single best prevention strategy is gradual ascent. Your body needs 1–3 days to adjust to each new elevation tier.
Safe Ascent Guidelines:
- Above 10,000 ft (3,048 m): Limit sleeping altitude increase to ≤1,000 ft (305 m) per day
- Add a rest day every 3,000 ft (915 m) gained
- Avoid flying directly into high-altitude destinations (e.g., Cuzco, Quito)
Example: If you fly into Denver (5,280 ft), spend a night before driving to 9,000 ft. If heading to Cuzco (11,200 ft), rest 24 hours before hiking.
Myth Busting: Physical fitness does not protect against AMS. Elite athletes are just as vulnerable.
Use “Climb High, Sleep Low” Strategy
This proven method helps accelerate acclimatization:
– Hike to a higher elevation during the day (e.g., 12,000 ft)
– Return to a lower altitude to sleep (e.g., 10,500 ft)
The stress of high exposure stimulates adaptation, while sleeping low allows recovery. Widely used on Everest expeditions and effective on trails like Mount Dana.
Pre-Acclimatize With Intermediate Stays
Spend 1–2 nights at 8,000–9,000 ft before attempting peaks above 13,000 ft. For example:
– Sleep in Mammoth Lakes before hiking Mount Dana (13,061 ft)
– Stay in Puno (12,545 ft) before visiting Lake Titicaca
Even a short acclimatization period significantly reduces AMS risk.
Medications That Prevent Altitude Sickness
Acetazolamide (Diamox): First-Line Defense
Acetazolamide is the most effective medication for preventing and treating AMS. It works by stimulating breathing, improving oxygen uptake.
Dosing:
- Prevention: 125 mg twice daily
- Start 24 hours before ascent
- Continue for 5 days at altitude
Why 125 mg? Lower dose reduces side effects while maintaining efficacy.
Side Effects:
- Tingling in fingers, toes, or lips
- Metallic taste (especially with carbonated drinks)
- Increased urination
- Rare: Severe allergic reaction (even without sulfa allergy)
Important: Do a test dose at home before your trip to check tolerance.
Who Should Take It?
- Anyone ascending rapidly above 10,000 ft
- History of AMS
- Flying directly to high elevation
Prescription required. Consult your doctor.
Dexamethasone: Emergency Backup
Dexamethasone is a steroid that reduces brain swelling and inflammation. Use only when descent is delayed or as rescue therapy.
Dosing:
- Treatment: 4 mg every 6 hours
- Prevention: 2 mg every 6 hours (short-term only)
Caution:
- Not for long-term use
- Requires tapering to avoid adrenal suppression
- Masks symptoms—don’t use to push higher
Best kept in emergency kits for HACE.
Ibuprofen for Headache Prevention
Surprisingly effective for AMS-related headaches.
- Dose: 600 mg daily (3 x 200 mg)
- Start 24 hours before ascent
Less effective than Diamox but useful for those who can’t take it.
Ginkgo Biloba: Limited Evidence
Some studies suggest 120 mg twice daily may reduce AMS incidence, but data is mixed. Not a reliable substitute for proven methods.
Bottom Line: Acetazolamide remains the gold standard. All medications should be discussed with a physician.
Optimize Hydration and Diet at Altitude
Drink 3–4 Liters of Water Daily
Dehydration worsens AMS symptoms and slows acclimatization. At altitude, you lose more water through breathing and sweat.
Hydration Tips:
- Aim for 3–4 quarts (3–4 liters) per day
- Monitor urine: Should be clear and frequent
- Add electrolytes (e.g., Nuun, Oral Rehydration Salts) to prevent hyponatremia
Avoid relying on thirst—your body’s signals are blunted at altitude.
Warning: Overhydration without electrolytes can cause dangerous low sodium (hyponatremia).
Eat High-Carb Meals Frequently
Carbohydrates require less oxygen to metabolize than fats or proteins, making them ideal fuel at altitude.
Ideal Diet:
- 70% of calories from carbs
- Whole grains, pasta, rice, fruits, honey
- Small, frequent meals to maintain energy
Avoid heavy, greasy foods that slow digestion.
Avoid Alcohol, Caffeine, and Sedatives
These substances interfere with acclimatization:
– Alcohol: Dehydrates and mimics AMS symptoms (headache, nausea)
– Caffeine: May contribute to dehydration; withdraw gradually if quitting
– Sleeping pills/tranquilizers: Suppress breathing—dangerous at altitude
Skip the après-hike beer until you’re back below 8,000 ft.
Treat Altitude Sickness in the Field

Mild AMS: Rest and Rehydrate
Most cases resolve with:
– Stopping ascent
– Hydration (3–4 L/day)
– Pain relief (ibuprofen or acetaminophen)
– Acetazolamide to speed recovery
Wait 24–72 hours before considering further ascent.
Moderate AMS: Descend 1,000 Feet
If symptoms persist or worsen:
– Descend 300–1,000 m (1,000–3,000 ft)
– Do not ascend again until fully recovered
– Use dexamethasone (4 mg every 6h) if descent delayed
Never ignore persistent vomiting or worsening headache.
Severe AMS, HAPE, or HACE: Immediate Descent
This is non-negotiable.
Action Steps:
- Descend 500–1,000 m (1,640–3,280 ft) immediately
- Evacuate to medical care
- Use supplemental oxygen (2–4 L/min) as bridge
- Deploy Gamow bag if descent delayed
Critical: No medication replaces descent. Oxygen and Gamow bags buy time—they don’t cure.
Use a Gamow Bag in Emergencies
The portable hyperbaric chamber simulates descent by increasing pressure around the patient.
How to Use:
- Place patient inside
- Inflate manually for 10 minutes
- Stay in bag for 1–2 hours
- Effect lasts up to 12 hours, allowing safer descent
Weighs ~14 lbs. Commonly carried on guided expeditions.
Recovery and Long-Term Outlook
Healing Timeline After Altitude Illness
- Mild AMS: Fully resolves in 1–3 days
- HAPE: May leave lingering cough or breathlessness for weeks
- HACE: Full recovery possible with prompt treatment
Most people return to normal activity within days to weeks.
Recurrence Risk Is High
If you’ve had AMS, HAPE, or HACE:
– Higher chance of recurrence on future trips
– Slower ascent and prophylactic Diamox recommended
– Consider pre-acclimatization strategies
No permanent damage occurs if treated early.
When to Seek Medical Follow-Up
See a doctor if:
– Symptoms persist after descent
– You were diagnosed with HAPE or HACE
– You used dexamethasone (requires tapering)
– You have underlying lung or heart conditions
Pulmonary function tests may be needed post-HAPE.
Final Note: Hiking altitude sickness is not a badge of toughness—it’s a physiological response that demands respect. By ascending slowly, recognizing symptoms early, and knowing when to descend, you can safely enjoy the world’s most breathtaking trails. Prepare, listen to your body, and remember the ultimate rule: Descend at the first sign of serious illness.